This article is the second in a series focused on wound care and pressure ulcers in nursing homes and long-term care settings. In the first post, we discussed how bedsores develop and when they may be a sign of neglect. In this article, we take a closer look at when a bedsore may cross the line into medical malpractice. In the coming weeks, we will continue to examine how these injuries progress, how they should be treated, and when they may raise serious concerns about the care being provided.
Not every bedsore is unavoidable. And not every bedsore is simply a medical condition.
In nursing homes and long-term care settings, pressure ulcers often develop in patients who are already vulnerable. But vulnerability does not eliminate responsibility. Healthcare providers are expected to recognize risk and respond to it with consistent, appropriate care.
The question is not just how a bedsore formed. It is whether it should have been prevented, identified earlier, or stopped from getting worse.
This is where the issue shifts.
In legal terms, medical malpractice occurs when a healthcare provider fails to meet the accepted standard of care, and that failure causes harm to a patient. In the context of pressure ulcers, that standard of care is well established and widely understood within the medical community.
When those standards are not followed, what begins as a medical concern may become something more serious. In some cases, it may be medical malpractice. Understanding that distinction is critical for families trying to make sense of what happened and whether it could have been avoided.

The Standard of Care in Nursing Homes
Nursing homes and healthcare providers are expected to follow established standards designed to prevent pressure ulcers and to treat them promptly if they develop.
These standards are not optional. They are a fundamental part of caring for residents, especially those who are immobile, medically fragile, or unable to care for themselves.
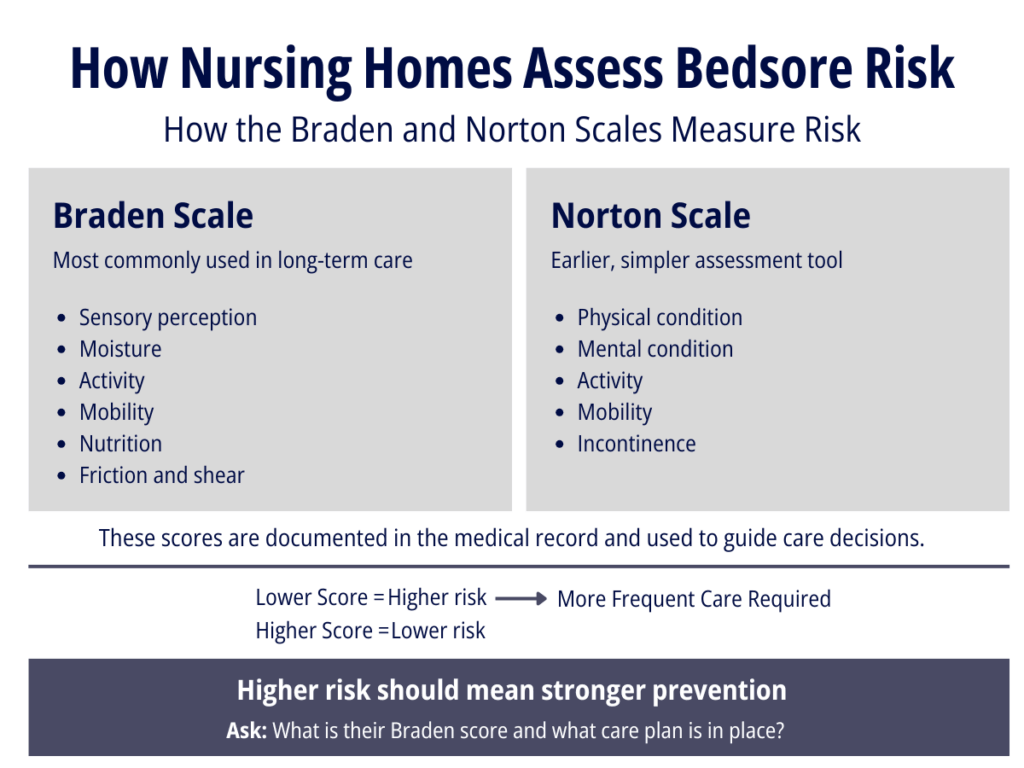
From the moment a resident is admitted, the facility should be evaluating their risk for skin breakdown and putting a plan in place to prevent it. That process is not based on guesswork. It is guided by standardized assessment tools, most commonly the Braden Scale or Norton Scale in long-term care settings. These tools measure factors such as mobility, moisture, nutrition, and a resident’s ability to reposition themselves, helping staff determine whether someone is at low or high risk for developing pressure ulcers.
This type of assessment should be performed upon admission and repeated as a resident’s condition changes. It is used to guide care decisions, including how frequently a resident should be repositioned, what type of support surfaces should be used, and how closely their skin should be monitored.
Learn more about the Braden and Norton Scales
A care plan based on that risk is expected to be carried out consistently, not simply documented in a chart.
Prevention requires active, ongoing care. Residents who cannot reposition themselves must be regularly turned. Their skin should be monitored for early signs of breakdown. Hygiene must be maintained, particularly for those experiencing incontinence, where prolonged moisture can quickly damage the skin. Nutrition and hydration must also be supported, as both play a direct role in maintaining skin integrity and promoting healing.
These are not extraordinary measures. They are basic components of appropriate care.
When they are followed, many pressure ulcers can be prevented or stopped before they become severe. When they are not, the risk of harm increases in ways that are often predictable and avoidable.
When Prevention Breaks Down
A bedsore may raise concerns about malpractice when these basic steps are not followed.
In many cases, the warning signs appear early. A resident may develop redness or irritation that indicates pressure is not being relieved. At that stage, intervention is critical. When appropriate steps are taken, the condition can often be stabilized or reversed.
When those steps are missed, delayed, or inconsistently applied, the injury can progress.
What families are often not told is that this progression is not inevitable. As noted in the first article, worsening stages of pressure ulcers frequently reflect a failure to intervene early or to monitor changes in the skin.
When a minor area of skin breakdown develops into a deep wound, it raises serious questions about whether the resident was receiving the level of care required.
When Treatment Should Prevent Deterioration
Even when a bedsore develops despite preventative efforts, the responsibility of the facility does not end there.
At that point, the focus shifts to treatment.
With proper wound care, monitoring, and medical oversight, a bedsore should begin to improve or, at a minimum, stop getting worse. Continued deterioration, especially rapid progression, is often a sign that something is not being done correctly.
This may involve delays in treatment, failure to follow physician orders, lack of proper wound care, lack of proper nutrition or hydration, or a breakdown in communication among staff.
In some cases, documentation may suggest that care was provided, but the condition of the wound tells a different story. A wound that continues to worsen over time is not simply a reflection of a resident’s overall health. It may be evidence that appropriate care was not provided.

The Role of Staffing and Facility Conditions
Bedsore-related malpractice is often tied to broader issues within a facility.
Understaffing is one of the most common factors. When there are not enough nurses or aides available, essential care tasks are delayed or missed altogether. Residents may not be repositioned as frequently as required. Basic hygiene may be postponed. Early signs of skin breakdown may go unnoticed.
Training is another critical issue. Preventing and treating pressure ulcers requires staff to recognize risk factors, understand care plans, and respond quickly to changes in a resident’s condition. Without proper training, even well-intentioned staff may fail to provide adequate care.
These systemic issues can create an environment where preventable injuries are more likely to occur.
The Impact on Dignity and Quality of Life
Beyond the medical implications, bedsore cases often involve a loss of dignity that families do not always see until the injury becomes severe.
Residents may be left in the same position for extended periods and forced to remain in soiled clothing or bedding for hours at a time. Pain may go unaddressed. Wounds may not be cleaned or treated as they should be.
These conditions are not simply unfortunate. They are often preventable and reflect a breakdown in basic caregiving. For many residents, especially those who cannot speak for themselves, these injuries occur quietly and without immediate visibility to family members.
Risk Does Not Remove Responsibility
Bedsore cases are often complex. Residents may have serious underlying health conditions, and facilities may argue that an injury was unavoidable.
However, the presence of risk does not remove responsibility.
The key question is whether the facility did what it was supposed to do to prevent harm and respond appropriately when a problem developed.
That is what separates an unavoidable medical issue from potential malpractice.

What Families Should Know
If your loved one developed a serious bedsore while in a nursing home or hospital, it is reasonable to ask how it happened and whether it could have been prevented.
A worsening wound, particularly one that progresses quickly or is not responding to treatment, may be a sign that basic standards of care were not met.
Understanding when a bedsore may be linked to medical malpractice is an important step in identifying whether something went wrong.
In the next article, we will examine what happens when pressure ulcers become infected and how these wounds can lead to serious, and sometimes life-threatening, complications.
Related Posts
Bedsores in Nursing Homes: When Pressure Ulcers May Be a Sign of Neglect
Understanding the Braden Scale and Norton Scale in Nursing Homes
Infected Bedsores, Sepsis, and Osteomyelitis: When Wounds Become Life-Threatening
Who is Responsible When a Bedsore Worsens After a Hospital or Nursing Home Transfer?
