Understanding how nursing homes assess risk using the Braden and Norton Scales
Pressure ulcers, also called bedsores, do not develop without warning.
In most cases, the risk can be identified in advance using standardized medical tools. In nursing homes and hospitals, the two most widely recognized tools are the Braden Scale and the Norton Scale.
These scales are not simply guidelines. They are part of how healthcare providers evaluate risk, make care decisions, and document what they know about a resident’s condition and risk.
Understanding how these tools work can help families recognize whether proper steps were taken to prevent harm.
What are the Braden and Norton Scales?
The Braden Scale and Norton Scale are clinical assessment tools used to determine a patient’s risk of developing pressure ulcers.
They are based on decades of medical research and are used in hospitals, nursing homes, and long-term care facilities across the United States and internationally.
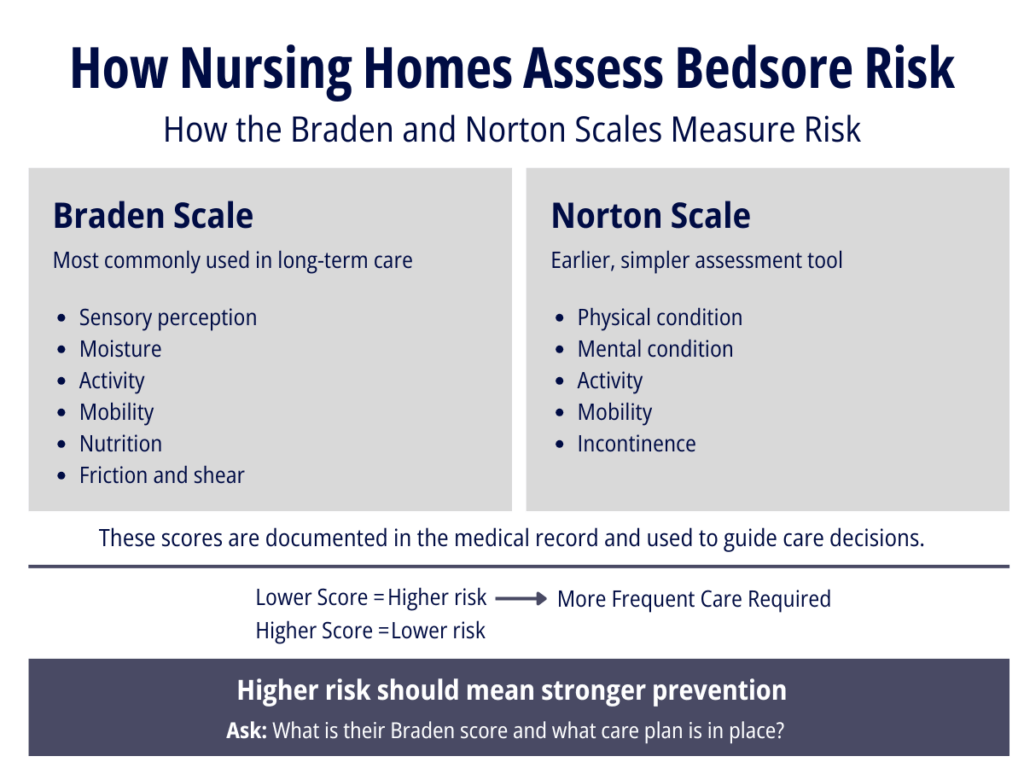
Each scale assigns a numerical score based on specific risk factors. That score helps guide care planning, including how frequently a resident should be repositioned, how closely their skin should be monitored, and what preventative measures should be put in place.
A lower score generally means a higher risk of developing a pressure ulcer. These assessments are typically documented in a resident’s medical record and updated over time.

Who developed these scales and where do the standards come from?
The Norton Scale was developed in the 1960s by Dr. Doreen Norton and colleagues in the United Kingdom. It was one of the first formal tools used to assess bedsore risk.
The Braden Scale was developed later, in the 1980s, by Dr. Barbara Braden and Dr. Nancy Bergstrom in the United States. It is now the most widely used risk assessment tool in long-term care settings.
While no single federal law requires a specific scale, nursing homes that participate in Medicare and Medicaid must follow federal regulations that require:
- Assessment of each resident’s risk for pressure ulcers
- Implementation of interventions to prevent skin breakdown
- Ongoing monitoring and documentation
The standards for pressure ulcer prevention and care are outlined in the CMS State Operations Manual.
In practice, facilities use tools like the Braden or Norton Scale to meet these requirements.
What is included in the Braden Scale?
The Braden Scale evaluates six areas that are directly related to skin breakdown and pressure injury risk:
- Sensory perception, or the ability to feel and respond to discomfort
- Moisture, including how often the skin is exposed to dampness
- Activity level
- Mobility, meaning the ability to change and control body position
- Nutrition
- Friction and shear, which refers to skin damage caused by rubbing or sliding against surfaces
Each category is scored, and the total score determines the resident’s level of risk. The Braden Scale is widely used in nursing homes because it provides a more detailed picture of the factors that contribute to pressure ulcers.
What is included in the Norton Scale?
The Norton Scale evaluates five areas:
- Physical condition
- Mental condition
- Activity
- Mobility
- Incontinence
Like the Braden Scale, each category is scored and combined into a total score that reflects the resident’s level of risk.
The Norton Scale is simpler and quicker to complete, but it is generally considered less detailed than the Braden Scale.
What are the differences between the Braden and Norton Scales?
Both scales are designed to answer the same question: how likely is a resident to develop a pressure ulcer?
The primary difference is the level of detail.
The Braden Scale focuses more closely on specific risk factors such as nutrition and skin moisture, which are directly tied to wound development. The Norton Scale takes a broader approach, focusing on overall physical and mental condition.
Because of this, many long-term care facilities prefer the Braden Scale, particularly for residents who require more complex care. In both cases, the goal is the same. Identify risk early and guide prevention.
Is one scale better than the other?
Clinical literature supports the use of the Braden Scale in long-term care settings because it provides more detailed information about risk factors that can be addressed through care planning.
However, both scales are considered acceptable tools.
The most important issue is not which scale is used. It is whether the assessment is performed correctly, updated regularly, and used to guide actual care.
Are all residents evaluated using these scales in Georgia?
Residents in Georgia nursing homes are expected to be assessed for pressure ulcer risk as part of their admission and ongoing care.
While the law does not require the use of a specific named scale, federal regulations require that facilities:
- Identify residents at risk
- Develop a plan to prevent pressure ulcers
- Reassess risk as conditions change
Facilities commonly use the Braden Scale to meet these requirements.
Do all nursing homes use these scales?
Most nursing homes use either the Braden Scale or the Norton Scale because they are widely accepted in the medical community.
Facilities may choose one tool over the other based on their internal policies, electronic medical record systems, and staff training.
Regardless of which tool is used, the responsibility remains the same. The facility must accurately assess risk and respond appropriately.
Do only residents with bedsores get evaluated?
Risk assessment is intended to prevent pressure ulcers, not respond to them after they develop.
Residents should be evaluated:
- Upon admission
- At regular intervals
- After any significant change in condition
If a facility is only assessing risk after a bedsore appears, that is a serious concern.
Who conducts these evaluations?
These assessments are typically performed by trained nursing staff, including registered nurses and licensed practical nurses.
They may also involve input from other members of the care team, particularly when developing or updating a care plan.
The results are documented in the resident’s medical record and used to guide daily care.

Are staff trained to perform these assessments?
Yes, they are expected to be.
Training is typically provided by the facility as part of staff onboarding and continuing education. This may include instruction on how to score each category, how to interpret results, and how to adjust care based on risk level.
However, the quality of that training can vary.
Inadequate training or inconsistent application of the scale can lead to incorrect scoring and inappropriate care decisions.
How should these scores affect care?
The purpose of these scales is not just to assign a number. It is to guide action.
When a resident is identified as high risk, the facility is expected to increase preventative measures. This may include more frequent repositioning, closer monitoring of the skin, specialized mattresses or cushions, and increased attention to hygiene and nutrition.
The higher the risk, the more aggressive the prevention should be.
If those steps are not taken, the risk identified by the scale can become a predictable outcome.
What happens if a resident is scored incorrectly?
An incorrect score can have serious consequences.
If a resident’s risk is underestimated, the care plan may not include the level of prevention needed. This can allow skin breakdown to occur or worsen.
If a score is not updated as a resident’s condition changes, the care plan may become outdated and ineffective.
In some cases, documentation may suggest that an assessment was performed, but the resident’s condition indicates that the risk was not properly evaluated or addressed.
What if there are differing opinions about a score?
Risk assessment is not always perfectly objective. Two clinicians may interpret certain factors differently.
However, this does not eliminate responsibility.
Facilities are expected to use clinical judgment, monitor changes over time, and adjust care as needed. If there is uncertainty, the safer approach is to treat the resident as higher risk and increase preventative measures.
Failure to do so can lead to avoidable harm.
Why this matters
The Braden and Norton Scales show what a facility knew about a resident’s risk and when they knew it. They also help show what should have been done in response.
When a resident develops a serious bedsore, these assessments often become a key part of understanding whether proper care was provided.
For families, knowing that these tools exist can change the conversation. It shifts the question from whether a bedsore was unavoidable to whether the risk was recognized and addressed.

What Families Can Ask and Request
Can families request an evaluation?
Yes. Families can request:
- A current risk assessment
- An updated care plan
- Clarification on how risk is being managed
Even if an assessment has already been done, asking for an updated evaluation is reasonable, especially if the resident’s condition has changed.
Can families request to see the results?
Yes. These assessments are part of the resident’s medical record, and under federal law (HIPAA), residents and their authorized representatives have the right to access those records, including risk assessment scores, care plans, and nursing notes.
What if a facility does not conduct an assessment?
This is a serious concern. Even private-pay facilities are expected to follow accepted standards of care. While they may not be directly governed by every CMS requirement, they are still expected to:
- Identify risk
- Take reasonable steps to prevent harm
Failure to conduct a risk assessment can be evidence that risk was not properly identified and preventative care was not implemented.
When to Consider Speaking with an Attorney
Pressure ulcer cases can be complex, particularly when they involve elderly residents with multiple medical conditions. Our attorneys have extensive experience handling these types of cases and understand how to evaluate whether proper standards of care were followed.
If you have questions about a loved one in a nursing home, or if someone you care about has been injured by a bedsore, we encourage you to reach out. You can call us at 706-354-4000 or complete our online contact form. We offer free case evaluations, and there is no fee unless we recover money for you in your case.